If you open a midwifery or obstetrics book, you will often find a description of the human female pelvis and birth canal, and of the normal progression of labour. This description is remarkably consistent across the literature, despite clear evidence of pelvic shape diversity across human populations. It is based on the most common pelvic morphology and labour progression in white women, and its use as a model for all women is problematic.
The shape of the birth canal varies across populations
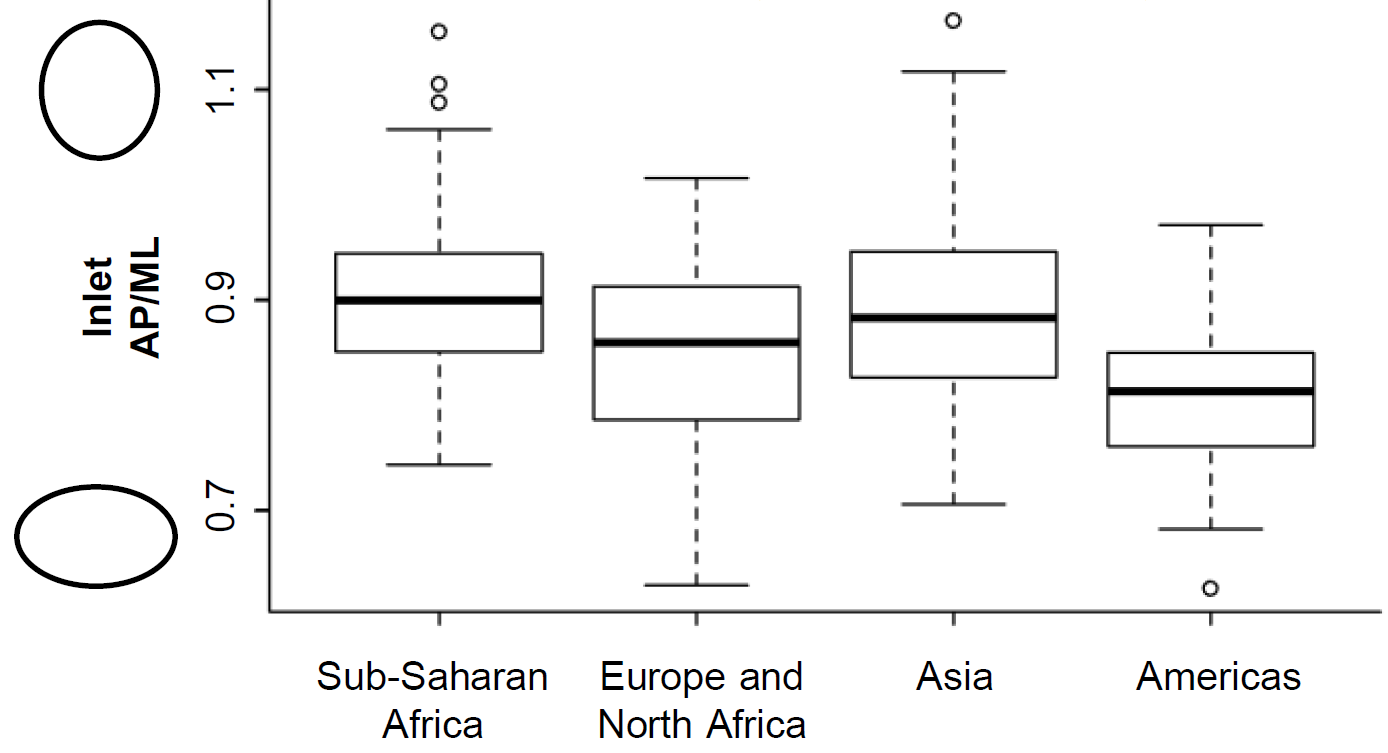
Women vary a lot in the shape of their birth canal, and this is not only true within a specific population, but also among populations from different parts of the world. Indeed, the average or most common shape of the birth canal differ across the world: sub-Saharan African and many Asian populations tend to have a round or anterior-posteriorly oval shape, while European and native American populations tend to have a transversally oval one (see figure). There is variation within continents and within each population, but this broad geographic pattern teaches us something important: using the average European pelvis as a model for all women, as is done in many obstetrics and midwifery books, is untenable. You can read about these findings in this paper and in this more accessible summary for The Science Breaker.
Inclusive maternal care cannot be based on white women’s physiology
Some understanding of women’s variation in the shape of the birth canal and its effects on labour started accumulating in the 1930s and 1940s, when the use of X-ray imaging permitted to study pelvic shape in living people (see figure). With the discovery of the damaging effects of X-ray, however, these studies stopped abruptly. A review of the evidence available until now shows that the process of labour, including the movement of the baby inside the canal and the likelihood of different interventions, differ depending on the mother’s pelvic shape. The current model of ‘normal’ labour, based on white women with a gynaecoid pelvis (see figure), does not necessarily apply to all women, especially if of other ethnic groups. In this paper, I make the case that the model of labour used in obstetrics and midwifery books is in fact discriminating against non-white women, whose labour is more likely to differ from the model and whose normal variation is more likely to be interpreted as abnormal. Together with several collaborators, I am planning a series of projects to evaluate whether this bias towards white women’s physiology is contributing to the higher maternal morbidity and mortality in women of other ethnicities in the UK. Some preliminary analyses of London NHS maternity data, funded by a UKRI-University of Roehampton Policy Support fund, shows differences in duration of labour, rates of labour interventions (especially focerps and c-section) and use of anaesthesia among ethnic groups, that need to be investigated further.
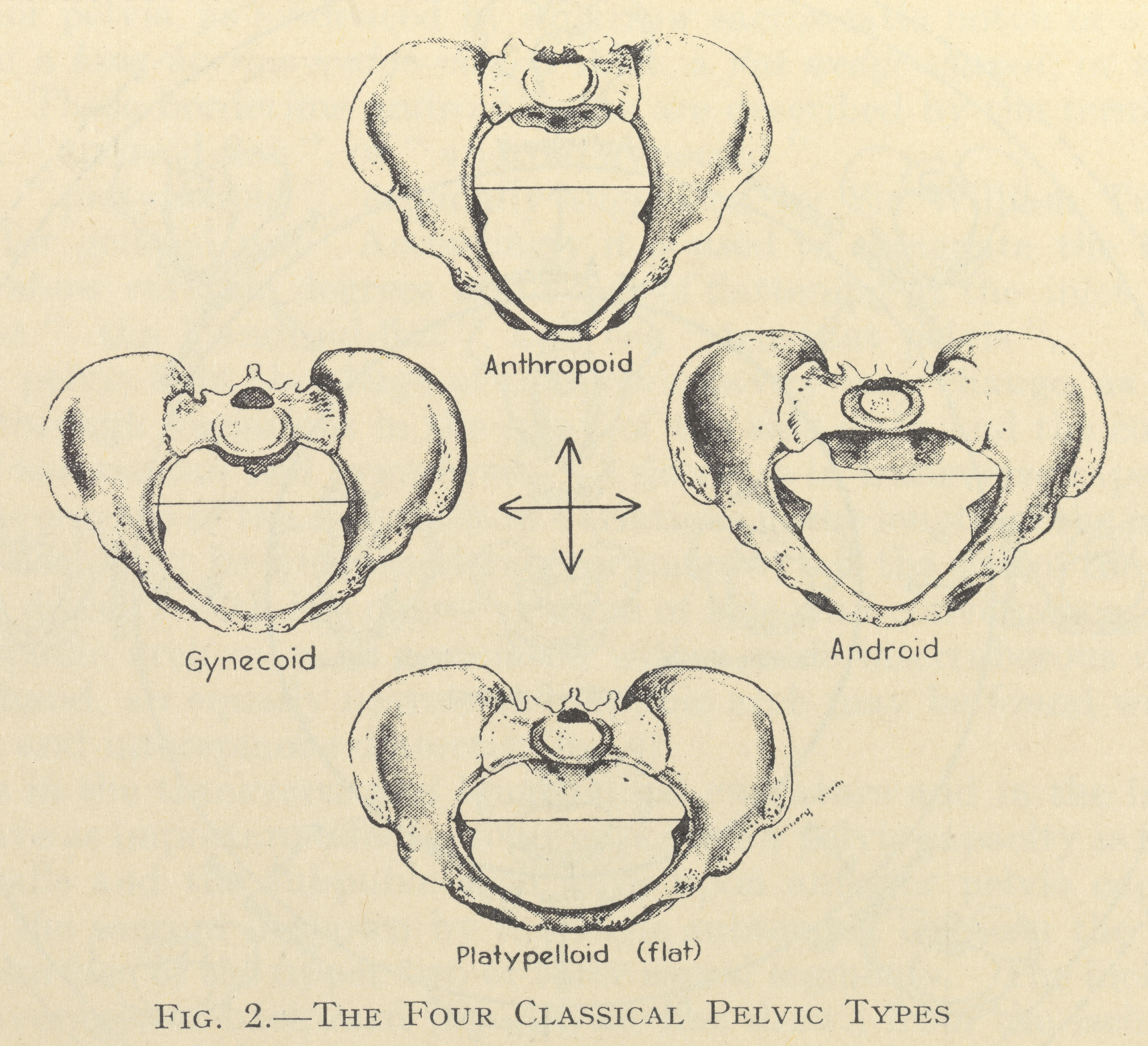
Caldwell and Moloy’s pelvic types (Caldwell and Moloy, 1938; from an unknown original source).
